Physicians Need High-Value HIE to Spur Adoption
By Shannon Vogel, Associate VP, Health Information Technology, and Ogechika Alozie, MD., Infectious Disease Specialist, Texas Medical Association
In 2009, Congress allocated millions of dollars to states to spur health information exchange (HIE) nationally by enacting the Health Information Technology and Economic Clinical Health (HITECH) Act. However, although health IT has progressed exponentially in the decade since the HITECH Act was implemented, physicians are still challenged when it comes to interoperability.
The HITECH Act included the Meaningful Use program that incentivized physicians to move from paper medical records into a digital format. The program required physicians to exchange patient information, but the bar was set low, and it was not difficult to apply exceptions. Now rebranded as Promoting Interoperability under the Centers for Medicare & Medicaid Services’ (CMS’) Quality Payment Program (QPP) authorized by the Medicare Access and CHIP Reauthorization Act (MACRA) of 2015, the program continues to push physicians and providers toward interoperability. Participants are required to share patient information in order to meet measures that earn performance points, which are then applied to a total QPP score that may result in payment incentives or penalties. The 21st Century Cures Act of 2016 sets the bar even higher as it requires prompt sharing of health information with patients, other physicians, and providers upon request, with very few exceptions.
The Struggle With Interoperability
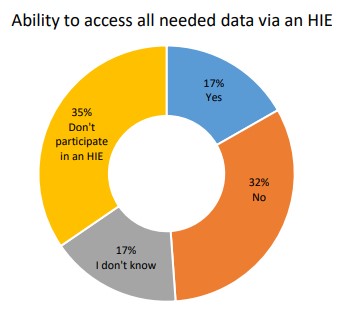
Physicians connected to an HIE are challenged by the value of the data received. A 2020 Texas Medical Association survey asked physicians if they are able to access all the data needed via an HIE when treating patients. Of the 1,303 respondents, only 17% said yes. In addition, low-value data can create extra work within the practice or be costly.
- Physicians do not always receive data sent or intended in the same or a consumable format. If the EHR cannot consume the data received, a PDF or similar attachment must be saved or information entered manually, or even worse, sometimes both. Interoperability should work seamlessly within the workflow and with such high value that it is the preferred option for sharing information.
- Information shared is not always necessary and relevant to what the medical team needs to take good care of the patient. Typically, what is necessary and relevant can be reduced to a couple of pages. However, physicians may receive hundreds of pages of information they must sift through to find what is necessary and relevant to deliver patient care. In addition to wasted time, the costs of electronically storing bloated records are significant, especially for physicians who own and operate a small practice with thin (if any) profit margins.
- Physicians in small practices do not typically have dedicated technology support. These physicians must have low-cost interoperability solutions that work well within the workflow and without a lot of extra technical effort.
- Physicians need assurances that they are sharing patient information with and among entities that embrace high standards for data privacy and security and not with weak links that risk exposing patient information.
Because of these difficulties, many physicians continue to rely on computer-generated faxing because it fits within the practice workflow, is secure, and doesn’t require a special and expensive interface. A recent data brief from the Office of the National Coordinator (ONC) indicates that about one-third (35%) of physicians used only fax, mail, or e-fax to share patient health information with physicians and providers outside of their organization (ONC cited the National Electronic Health Record Survey, 2019).
As physicians evaluate various interoperability choices, some starting with the low-cost option of Direct Secure Messaging, which can be considered as a secure email. To send a Direct message, a physician must have a Direct protocol address and know the intended recipient’s address. Messages are sent in a secure, encrypted, HIPAA-compliant manner. CMS now requires that physicians update their National Plan and Provider Enumeration System account with a digital address, and a Direct Secure Messaging address satisfies the requirement. Unfortunately, physicians are not always well informed about how to get a Direct address and how to adjust and manage the practice workflow to accommodate sending and receiving messages. A good first step is to ask EHR vendors. A good second step is to ask the local HIE.
The Technology Is There – Let’s Use It
To spur interoperability, capabilities should be baked into the EHR so that once physicians sign the necessary user agreement(s), the spigot is activated, and bi-directional exchange happens within the workflow. By leveraging national networks and applying the United States Core Data for Interoperability (USCDI) and its accompanying standards, the developer community could help physicians exchange health information in a manner that does not require costly interfaces or a lot of technical effort. The technology does exist to accomplish HIE better, faster, and cheaper. The Trusted Exchange Framework and Common Agreement, or TEFCA, is helping standardize the rules of the HIE road. Industry efforts are coalescing in such a way that medical practices should be able to have one bi-directional connection that intelligently disseminates clinical data across the networks in a standardized way. High-value HIE allows physicians and providers to have relevant information, organized meaningfully, about the right patient at the point of care to make good clinical decisions.
Physicians are increasingly frustrated with the inefficiencies of digitized records requiring extra time spent on technology-related challenges that take away from patient care. EHRs have always promised increased care quality, patient safety, and greater efficiency. It behooves us as health care technologists to keep those goals top of mind for better patient care, which requires working creatively and collaboratively to achieve them.