
Jet Fuel For Your Clinical Documentation Integrity Program
By Pamela Arora, SVP CIO and Katherine Lusk, Chief Health Information Management & Exchange Officer, Children’s Health
In 2012, Children’s HealthSM faced two significant environmental changes that held the potential to impact provider workflow vis-a-vis additional documentation requirements. And if these changes were not handled well, they could result in a significant negative impact to provider efficiency, clinical communication, and revenue capture. With the possible financial impact being in the millions, we needed to “fuel up” for these changes. What were they?
- Texas was moving to Prospective Payment System (PPS) for Medicaid inpatients Sept. 1, 2013
- Roll out of the International Classification of Diseases Version 10 on Oct. 1, 2015
Being an organization that seeks to leverage the power of technology tools to improve care delivery and outcomes, we thought this challenge represented a perfect opportunity to draw on the collaborative spirit of our team members, to develop processes that would enable us to meet the requirements of PPS and ICD-10, and employ the robust technology tools we have deployed across our organization.
This initiative resulted in Children’s Health in Dallas rolling out a Clinical Documentation Integrity Program that was fueled by a combination of technology, data analytics, and process changes that ultimately helped us increase overall case mix index (without additional employees), improved clinical communication, and streamlined provider documentation.

People and Process:
We assembled a multidisciplinary workgroup comprised of physicians, advance practice nurses, nutrition, coders and clinical documentation integrity specialists. The work effort began with the team defining the problem and conducting an extensive literature review. Our plan was to begin the process with our Gastrointestinal division and then expand the project to all departments. As such, we secured a physician champion from the gastrointestinal division and sought participation from disciplines to serve as subject matter experts. The clinical documentation integrity specialist facilitated the meetings, pulled the information together and wrote/managed the multiple drafts. Then the document was socialized, which enabled us to receive valuable feedback. The socialization process included meeting with providers one-on-one, department meetings, case studies, posters, and lunch-and-learn engagement. This resulted in extensive changes to the document, which was then triangulated against literature review to ensure we were maintaining a solid scientific base. With the vetting process being tied to scientific evidence, we were able to accomplish and sustain the culture change necessary to gain adoption. The Health Information Management (HIM) team served as the leadership force in the project, with the IT team supporting the “power pack” behind the solution that was embedded in the workflow.
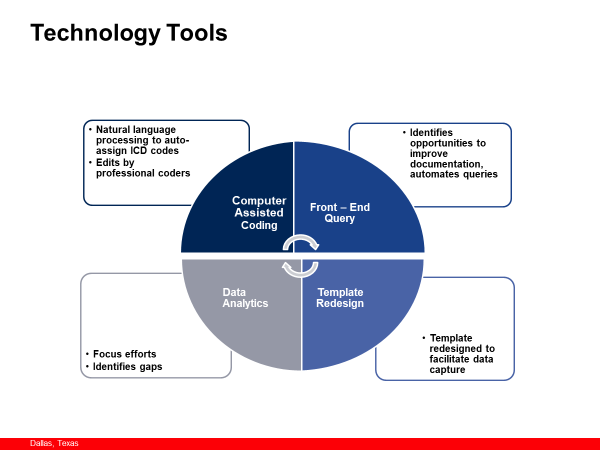
The Power Behind the Program (Technology)
Children’s Health used its electronic medical record (EMR) and clinical decision support tools to support this initiative. The EMR tools used included the clinical documentation integrity application, template redesign, and reporting tools. The clinical decision support tools included computer assisted coding, APR-DRG enhancer, and auto-generated queries. Clinical communication was improved with the increased capture of co-morbid conditions, and provider documentation was streamlined to improve efficiency without the need for additional full-time employees (FTEs) for the effort. Implementation of the EMR allowed us to shift staff that had previously performed other roles into clinical documentation integrity (CDI) positions. There were also additional benefits to case management department.
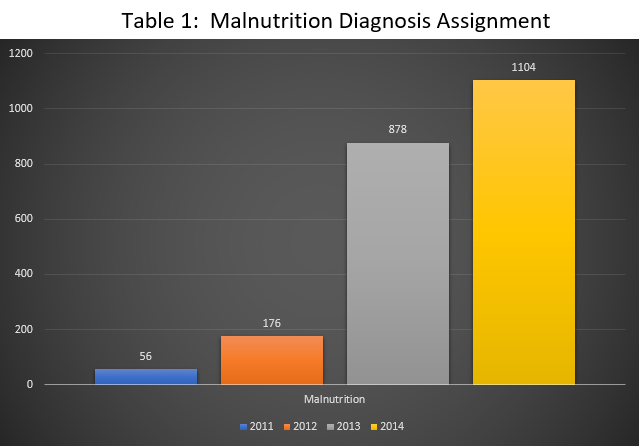
The technology was finalized in 2013, clinical definitions were published on an internal website dedicated to physicians and circulated to the medical community. For example, in 2013, there were 878 inpatients with the diagnosis of malnutrition and 1,104 in 2014. We believe these statistics are the result of acceptance across the disciplines and recognition of the value of a standard definition for malnutrition in the pediatric population. The table below illustrates the progression of the process, growing acceptance, and sustainability.
The following matrix demonstrates the Documentation Integrity rollout of People, Processes, Technology, and Tools:
| 2012 | Data analysis, identified opportunities, and developed communication plan. |
| Computer assisted coding implemented | |
| Standardized pediatric queries built as Smart Notes | |
| 2013 | Malnutrition clinical definition |
| Template redesign to capture specificity while streamlining documentation started with oncology and worked incrementally thru house. | |
| Reports to identify opportunities for questions; hyponatremia, CHF, anemia, respiratory failure, cardiogenic shock, malnutrition, obesity, diabetes, sepsis, and epilepsy | |
| Anemia clinical definition | |
| Heart failure clinical definition | |
| APR DRG with Severity of Illness and expected length of stay in header | |
| Respiratory failure clinical definition | |
| 2014 | Renal & respiratory failure clinical definitions |
| Queries integrated into HIM deficiency process that turned red at 24 hours | |
| Asthma clinical definition | |
| 2015 | Template redesign |
| Epilepsy clinical definition | |
| Encephalopathy & Coma clinical definitions | |
| 2016 | Anemia, renal failure, obesity, sepsis & epilepsy clinical definitions |
| BPAs for invalid diagnoses | |
| Automated specificity query pilot | |
| Pancreatitis & Encephalopathy clinical definitions | |
| 2017 | Automated specificity query incremental roll-out |
| Query redesign with links to clinical definition | |
| 2018 | Clinical Definition Opioid Disorder / Misuse |
Communication Plan
Initial discussions took place in which the Chief Health Information Management and Exchange Officer and the Chief Information Officer met with the Division Chiefs, and Chair of Pediatrics to lay out the planned approach of “people, processes, and tools” in this initiative. Once these senior leaders were comfortable with the tools and approach, the communication planning began. A project of this magnitude required a solid communication plan in which we crafted and targeted our communication by discipline, providing routine updates to Division Chiefs, Health Electronic Record / Health Information Management members and Utilization Review Committee members. From there, we asked these team members to cascade this information to their peers. At first, communication was provided monthly until we determined an appropriate cadence to the messages. Now, these updates are delivered quarterly. We sought to augment our communications with a more “grass roots” approach through numerous lunch-and-learn events within departments. We also conducted (and continue to conduct) face to face meetings with providers as needed. In addition, the team participated in clinical rounding; however, after discussion with medical staff, we determined that this wasn’t the most appropriate vehicle for this communication. Rather, the team found that it was most effective when monthly communication and engagement was reported to the Health Information Management / Health Electronic Record Committee and Utilization Review Committee.
Outcomes
In the first year of the Clinical Documentation Integrity program, prospective payment for Children’s Health showed an increase in reimbursement rather than a decrease—this was an expected result. Case Mix Index continued to increase annually until 2016, when we reached a plateau. Bill drop days declined from 5 days in 2011 to 3.5 days in 2016. Of note, however, is the fact that as of 2017, the bill drop days has increased to 5 days due to other factors. The increase in CMI was FTE-neutral in that no new FTEs were needed as a result of the CDI initiative.
With implementation of computer-assisted coding, data analysis showed that coders captured an average of two additional diagnosis codes per inpatient discharge, which resulted in an increase in case mix index (CMI) of 7% prior to clinical documentation team staffing. These results proved to us that technology is a big contributor to improved documentation, and to this day, CMI continues to grow with clinical documentation team staffing.
As a specialty referral system, many of our providers see a set population of patients with similar documentation requirements. This presented an opportunity for us to standardize templates for these patient populations, due to the general lack of variation in documentation. The design process focused on evaluating workflow and providing drop downs with co-morbid conditions that were usually present in the population. Once we rolled out standardized templates, the CMI increased, documentation was completed in less time, and provider satisfaction improved.
Our analysis showed a prevalence of documenting manifestations of the disease process rather than documenting classifiable conditions. With this understanding, the multidisciplinary team developed standardized clinical definitions, which led to agreement across the medical staff on diagnosing co-morbid conditions, improving efficiency of clinical communication and increasing CMI. The net result is that clinical communication was streamlined and improved by standardization.
Additionally, our analysis showed providers were not consistently capturing co-morbid conditions that were associated with the principal diagnosis. This finding led to Children’s Health and the team to work with providers to redesign their templates, resulting in a more effective means of capturing these diagnoses without adding to the standard workflow.
Case managers have an increased awareness of APR-DRGs, severity of illness and expected length of stay, allowing them to be more actively engaged in assuring complete documentation.
Lessons Learned:
- The value of the CDI team working closely with the medical staff, leveraging focused communication, is immediately evident at month end when there is a drop.
- Monitoring KPIs and reacting/responding quickly assures no slippage.
- Keeping material fresh and relevant is the key.
- Provider response to queries time decreased immediately when providers were given a visual queue that a query was older than 24 hours (measured in June of 2014 and then again June of 2017 following the query redesign). Automated queries on specificity in 2018 also showed the same trend.
- Continued refreshing and packaging of the material within the provider workspace has allowed sustained improvements in our documentation.
Clinical documentation integrity can improve provider workflow, assure accurate population representation, support more complete clinical communication, and provide positive financial impact. Our CDI program has shown the test of time, accurately representing the acuity of our patient population.
Scenario: How more accurate CMI impacts the bottom line
To understand the impact, you need to know that total reimbursement is figured by multiplying an organization’s base rate by the CMI weight (Base Rate x CMI Weight).
Each hospital’s base rate is different, so we’ll use hypothetical numbers to illustrate the impact. Let’s say that your base rate is $10K. Under this scenario (using the CMI example below), in 2012, our organization would have been reimbursed $17.6K per patient ($10K x 1.76), but in 2019, the same patient population would be reimbursed at $26.1K ($10K x 2.61), an increase of nearly $10K. While this is a general illustration, it’s easy to see how even a small incremental change in CMI accuracy can result in significant impact to your organization’s bottom line.
Our goal is for programs to accurately reflect acuity and capture co-morbid conditions. One example is our nutrition program, which expanded based on our ability to capture more frequently the diagnosis of malnutrition. Ultimately, our efforts have helped us better support the unique healthcare needs of our community.
Summary:
- A multidisciplinary clinical documentation integrity program supports success
- Technology underpinning is fundamental
- Restructuring templates can more accurately reflect patient acuity, streamline documentation efficiency, and improve provider satisfaction
- Automated queries in workflow facilitates provider response
- KPIs and data analytics keep you on track


